JOINTS 2024;
2: e1058
DOI: 10.26355/joints_20247_1058
Potential benefits of oral hyaluronic acid and Boswellia serrata extract in patients with mild to moderate knee osteoarthritis
Topic: Knee
Category: Original article
Abstract
OBJECTIVE: Knee osteoarthritis (OA) affects millions of people. The role of oral supplements among conservative treatments for knee OA is still debated. This prospective observational study evaluates the efficacy of oral supplements of hyaluronic acid and Boswellia serrata extract in reducing pain and improving joint range of motion in patients with mild-moderate knee OA.
PATIENTS AND METHODS: Forty patients (24 women and 16 men), with a mean age of 67.6 ± 7.9, took one tablet of oral supplement based on hyaluronic acid 300 mg + Boswellia serrata extract 100 mg per day for 60 consecutive days. The follow-up lasted six months. After 1 (T1), 3 (T2) and 6 (T3) months, each patient underwent clinical consultation with pain and knee function assessment using specific scores [(Visual Analog Scale (VAS), Knee Injury and Osteoarthritis Outcome Score (KOOS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and the International Knee Documentation Committee (IKDC)]. Finally, during the last consultation, the degree of patient satisfaction was assessed (on a scale of 0 to 10).
RESULTS: Two of the 40 patients dropped out of the study (5% dropout rate). The VAS showed a statistically significant improvement (p < 0.001) between the first and subsequent visits, with a clear reduction in pain between T1 and T2. The KOOS improved at each visit, with statistically significant results (p < 0.001) between T0 and T1 and between T2 and T3. The WOMAC showed statistically significant improvements (p < 0.001) between the first and all subsequent consultations, while between T2 and T3, the results showed a non-statistically significant reduction in the score. The IKDC score showed statistically significant improvements (p < 0.001) between the first and all subsequent consultations, with non-statistically significant differences between T1 and T2, T1 and T3, T2 and T3. Finally, the degree of satisfaction was 8.1 ± 1.4.
CONCLUSIONS: Oral administration of hyaluronic acid and Boswellia serrata extract decreases pain and improves knee function in patients with mild to moderate knee OA.
Introduction
Conservative treatment strategies for knee osteoarthritis (OA) are twofold: pain control and function restoration. Several treatment modalities, often in combination, can be used to achieve these goals.
Oral nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen are commonly used, depending on the patient’s cardiovascular comorbidities, for short periods of time, given their side effects1,2. In addition to oral therapy, intra-articular injection therapy with corticosteroids, hyaluronic acid (HA), platelet-rich plasma (PRP) and mesenchymal stem cells is used. Depending on the type of molecule used, intra-articular therapies provide short- to medium-term benefits, although they often require multiple injections3-6.
Given the increasing incidence of knee OA and problems with tolerability and toxicity, especially in elderly patients with conservative pharmacologic and injectable therapies, non-pharmacologic oral supplements are increasingly being studied1,2,7. Herbal agents such as Boswellia serrata have been investigated for safety and efficacy in the management of knee osteoarthritis. Different studies8-10 have demonstrated the effectiveness of oral supplementation of Boswellia serrata in reducing pain, improving physical function, and decreasing inflammation in patients with knee osteoarthritis.
Also, studies11-15 focused on oral supplementation of HA, a high-molecular-weight molecule normally found in cartilage and synovial fluid that acts as a viscoelastic lubricant and cellular regulator through protein binding. Its efficacy appears to be partly explained by its anti-inflammatory role and as a promoter of extracellular matrix protein synthesis, thus contributing to the maintenance of normal articular cartilage thickness.
Because of these mechanisms of action, combined with fewer side effects than NSAIDs and acetaminophen, oral supplements based on Boswellia serrata and hyaluronic acid can be a viable alternative for patients suffering from knee OA.
The aim of this study was to evaluate the efficacy of oral hyaluronic acid 300 mg + Boswellia serrata extract 100 mg during a 6-month follow-up period in reducing pain and improving knee function in patients older than 45 years with mild to moderate primary knee OA.
Patients and Methods
A prospective cohort study was conducted in 2022 at our institution (Sant’Andrea University Hospital). Patients were included if they presented with mild to moderate primary knee OA (according to Kellgren Lawrence and Ahlback classification: stage I-II) and age ≥ 45 years.
Patients were excluded if they presented with severe knee OA (stage III-IV), received an ipsilateral intraarticular injection in the prior six months, underwent previous ipsilateral surgical procedures, had autoimmune disorders, or were unwilling to be enrolled in the study. Patients were excluded from the study if they underwent other pharmacologic or surgical therapies for the treatment of knee OA during the study period.
Each participant took one tablet per day of oral hyaluronic acid 300 mg + Boswellia serrata extract 100 mg supplement for a duration of 60 days. The patients were asked to record diaries to track patient compliance.
The study was authorized by the local Ethics Committee and performed in line with the Ethical Standards of the 1975 Declaration of Helsinki, as revised in 2013.
Physiotherapy
A standardized physiotherapy protocol was prescribed. The initial phase focused on pain management, employing modalities such as cold therapy and transcutaneous electrical nerve stimulation (TENS). Gentle range-of-motion exercises were introduced to maintain joint mobility without exacerbating symptoms. As patients progressed, strengthening exercises targeting the quadriceps, hamstrings, and calf muscles were integrated into the regimen. Proprioceptive exercises, including single-leg stance and closed-chain activities, were introduced to promote joint stability. The protocol also emphasized functional training tailored to individual patient needs, aiming to restore daily activities without pain or discomfort. Patient education on joint protection and activity modification was also incorporated throughout the therapeutic sessions. The duration and frequency of the sessions were determined based on individual patient requirements and clinical response but typically consisted of twice-weekly sessions for six to eight weeks.
Clinical Evaluation
The effects of this oral supplementation were evaluated longitudinally at intervals of one, three, and six months after initiation.
Clinical assessments included recording the body weight. At each endpoint, self-reported metrics – including the Visual Analog Scale (VAS), Knee Injury and Osteoarthritis Outcome Score (KOOS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and the International Knee Documentation Committee (IKDC) scale – were employed for the evaluation of pain indices and knee function prior to the treatment (T0) and at one (T1), three- (T3), and six-months (T3) post-initiation. The final follow-up included an evaluation of patient satisfaction scaled from 1 to 10.
Statistical Analysis
All analyses were performed with the SPSS® Statistics software (version 27.0.1.0; IBM Corp., Armonk, NY, USA). Statistical significance was set at p < 0.05. Descriptive data were analyzed for the entire patient cohort. Descriptive data analyses were conducted depending on the nature of the considered criteria. For quantitative data, this included the number of observed values (and missing values, if any), mean, SD, median, and minimum and maximum. For qualitative data, this included the number of observed and missing values and the number and percentage of patients per class. To assess differences between the four endpoints, a one-way repeated measures analysis of variance was conducted; significance values were adjusted according to Bonferroni’s correction for multiple tests.
Results
Of the 40 patients initially included in the study, 2 (5%) dropped out. All remaining patients took one tablet of the supplement daily for 60 days. The age of the enrolled patients ranged from 50 to 81, with a mean of 67.6 ± 7.9 years and a median Kellgren-Lawrence score of 2. Table 1 shows the demographic characteristics of the study population.
Table 1. Demographic data of the population included in the study. Values are reported as number (%) or mean ± standard deviation (SD).
| Sex, n (%) | |||
| Male | 16 | (40) | |
| Female | 24 | (60) | |
| Side, n (%) | |||
| Right | 25 | (62.5) | |
| Left | 15 | (37.5) | |
| Kellgren-Lawrence grade, n (%) | |||
| 1 | 12 | (30) | |
| 2 | 20 | (50) | |
| 3 | 8 | (20) | |
| Age, mean ± SD | 67.6 | ± 7.9 | |
| Height, mean ± SD | 168.2 | ± 8.9 | |
| Weight, mean ± SD | 78.9 | ± 13.3 | |
The study population’s body weight significantly decreased over the study period: T0, mean 78.9 kg; T1, mean 71 kg (p = 0.005). At the final endpoint, the mean satisfaction score was 8.1 ± 1.4 (range, 5-10). An analysis of the VAS, KOOS, WOMAC, and IKDC at the four endpoints was performed and is presented in Table 2.
| Pairwise Comparison | ||||||
| Mean | SD | T1 | T2 | T3 | ||
| VAS | ||||||
| T0 | 6.65 | 1.78 | < 0.001 | < 0.001 | < 0.001 | |
| T1 | 4.85 | 1.82 | 0.001 | 0.069 | ||
| T2 | 3.58 | 13.63 | 0.166 | |||
| T3 | 3.85 | 2.13 | ||||
| KOOS | ||||||
| T0 | 72.28 | 8.67 | < 0.001 | < 0.001 | 0.009 | |
| T1 | 73.36 | 13.59 | 0.999 | 0.488 | ||
| T2 | 73 | 13.59 | 0.488 | |||
| T3 | 75.03 | 9.44 | ||||
| WOMAC | ||||||
| T0 | 67.67 | 9.88 | < 0.001 | < 0.001 | < 0.001 | |
| T1 | 75.26 | 9.54 | 0.011 | 0.411 | ||
| T2 | 78.10 | 9.44 | 0.083 | |||
| T3 | 77 | 9.62 | ||||
| IKDC | ||||||
| T0 | 62.96 | 11.81 | < 0.001 | < 0.001 | < 0.001 | |
| T1 | 70.95 | 10.64 | 0.076 | 0.319 | ||
| T2 | 68.78 | 10.43 | 0.436 | |||
| T3 | 71 | 9.67 | ||||
The boldface indicates statistical significance. SD, Standard Deviation.
VAS
Regarding VAS, a steady decrease in pain was observed from the start of treatment, with a significantly improved score between T0 and the other endpoints (p < 0.001). In addition, an improvement was noted between T1 and T2 (p = 0.001) (Figure 1).
Figure 1. Visual Analog Scale (VAS) scores at the four endpoints.
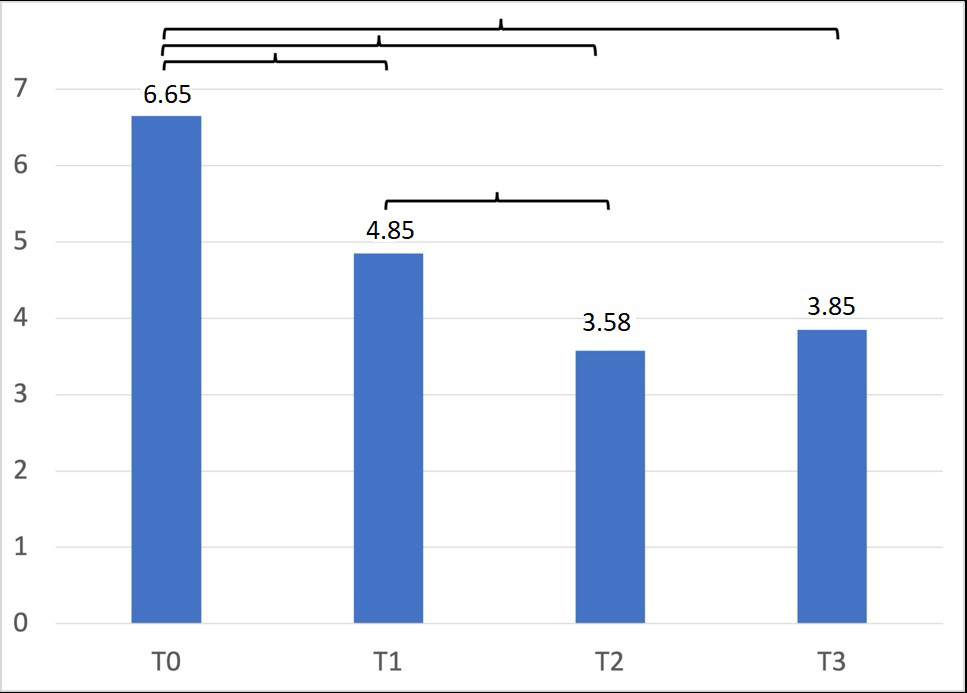
The presence of curly brackets indicates a statistically significant difference.
KOOS
There was a statistically significant steady increase in KOOS score at the various endpoints (p < 0.001).
Scores were significantly improved between T0 and T1 (p < 0.001), T2 (p < 0.001) and T3 (p = 0.009) (Figure 2).
Figure 2. Knee Injury and Osteoarthritis Outcome Score (KOOS) scores at the four endpoints.
The presence of curly brackets indicates a statistically significant difference.
WOMAC
The WOMAC score showed a significant improvement between T0 and T1 (p < 0.001), T2 (p < 0.001) and T3 (p < 0.001), and between T1 and T2 (p < 0.001), with a non-significant decrease from T2 to T3 (p = 0.436) (Figure 3).
Figure 3. Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores at the four endpoints.
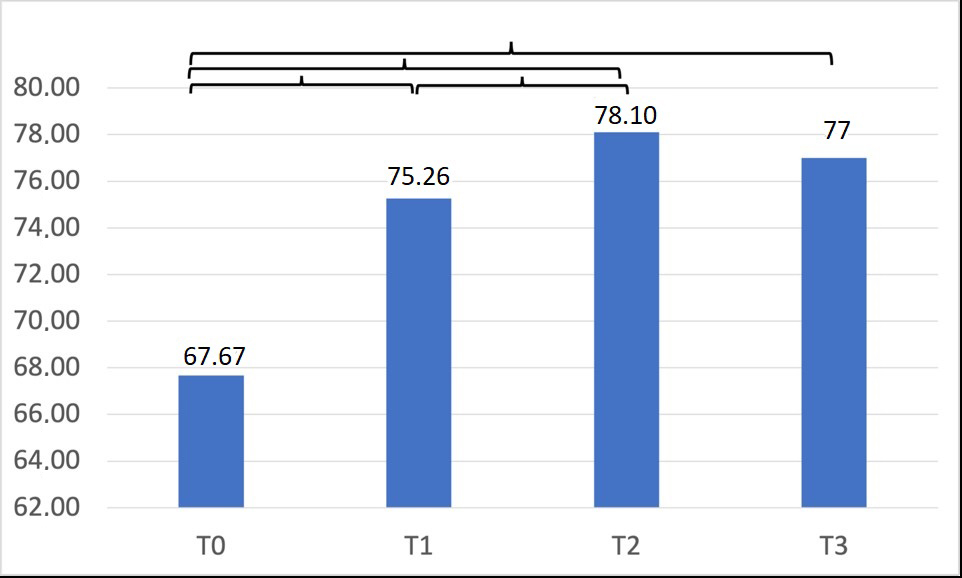
The presence of curly brackets indicates a statistically significant difference.
IKDC
There was no linear progression of scores for the IKDC score. All measurements taken were significantly increased from T0 (p < 0.001), but no other differences were shown. In addition, the score fell between T1 and T2 and then rose again at T3 (Figure 4).
Figure 4. International Knee Documentation Committee (IKDC) score at the four endpoints.
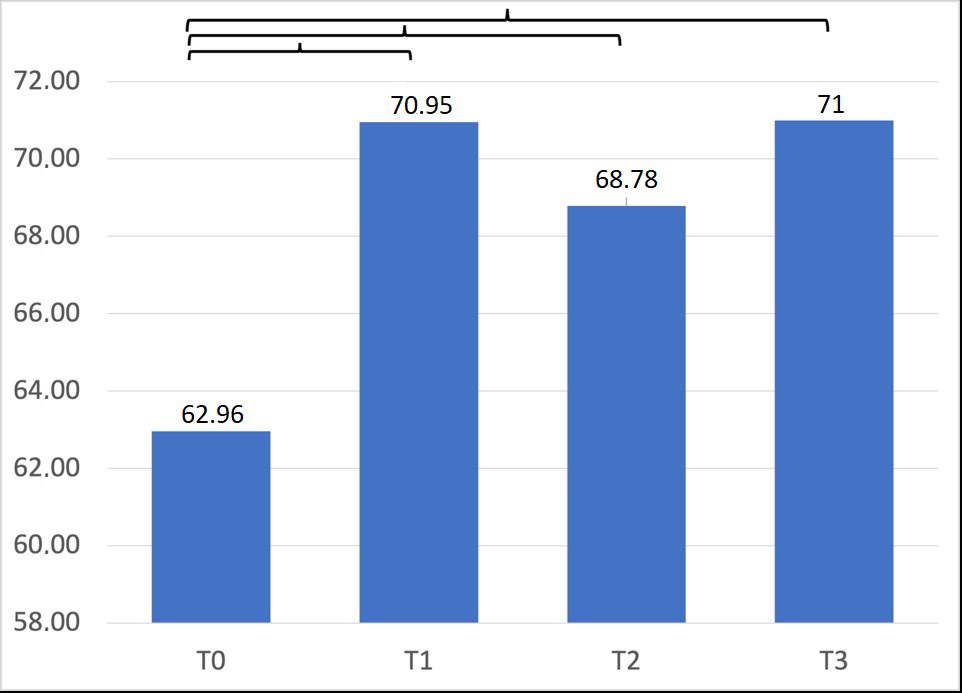
The presence of curly brackets indicates a statistically significant difference.
Discussion
The main result of this observational study is that taking one tablet of hyaluronic acid and Boswellia serrata extract daily for at least 60 days can effectively reduce pain and improve knee function in patients with mild to moderate knee osteoarthritis in the short term.
HA is an organic compound naturally synthesized by fibroblasts that maintains the structural and functional properties of extracellular matrix fluids, such as tissue protection and repair11. HA improves synovial fluid elasticity and viscosity, decreases the release of pain-producing neuropeptides and proinflammatory mediators and produces anti-inflammatory effects such as interleukin (IL)-1 suppression16-19. Boswellic acid is the active ingredient in Boswellia serrata. Boswellia, containing 10% Acetyl-Keto-β-Boswellic acid (AKBA), is useful for joint function. AKBA is a boswellic acid with strong pharmacological activity: it has anti-inflammatory properties, is an inhibitor of the lipoxygenase pathway, has anti-arthritis properties, and improves pain and physical function. A systematic review and meta-analysis20 showed that Boswellia and its extract may relieve pain and stiffness and improve joint function, potentially being a beneficial drug for patients with OA. For these reasons, the combination of hyaluronic acid and Boswellia, exploiting the synergistic beneficial properties of both substances, would positively impact pain.
Ricci et al21 compared oral and intra-articular hyaluronic acid, showing short-term follow-up improvements in function and knee pain, measured by a reduction in the VAS score and an improvement in the American Knee Society Score (AKSS) for both administration routes. However, in the elderly population, better results were obtained with oral administration of HA.
Regarding pain, as assessed by the VAS score, we observed a statistically significant decrease over time, with a constant decrease from the start of the treatment and a significant improvement between T0 and the other endpoints (p < 0.001). This improvement was present from the first month, and although pain did not improve in a statistically significant manner between T2 and T3, it did not return to pre-treatment levels on the VAS scale. In the future, it would be useful to evaluate the effects of a possible new course of supplementation on pain. Jensen et al22 analyzed the effects of oral hyaluronic acid supplementation in 70 patients. A reduction in pain was seen as early as two weeks, consistent with the data in our study.
Regarding knee function (analyzed by KOOS, WOMAC and IKDC scores), we observed a constant increase in the KOOS score across the various endpoints, with statistically significant overall progression (p < 0.001); a non-constant trend in the WOMAC score with a significant improvement between T0 and T1 (p < 0.001), T2 (p < 0.001) and T3 (p < 0.001) and between T1 and T2 (p < 0.001), without a significant decrease from T2 to T3 (p = 0.436); a non-linear progression in IKDC score in which all measurements made were significantly increased from T0 (p < 0.001).
Improvements in function and pain are also to be correlated with a reduction in the inflammatory state of the joint, as shown by the analysis of synovial fluid conducted on 40 patients taking an oral preparation containing HA for 3 months23. This improvement also leads to a reduction in the intake of other medications with various side effects, as opposed to HA supplementation, which appears to be much safer23,24.
Our results seem to be in line with two previous studies12,13, although these studies also showed that patients younger than 70 years and with an initial VAS of less than 3 had better outcomes with oral HA intake.
We evidenced encouraging results at the 6-month follow-up after 60 days of oral administration of one tablet/day based on hyaluronic acid and Boswellia serrata extract. Pain decreased immediately, reaching minimum levels three months (T2) after the first administration of the integration.
Limitations
The relatively small sample size, the short-term follow-up, and the absence of a control group limit the generalizability of our results. In addition, the study did not control for potential confounding factors such as lifestyle changes, body weight loss and other therapies, which may have influenced the outcomes. Due to the lack of a physical therapy center at our institution, it was also not possible to directly assess whether patients actually followed the prescribed physical therapy protocol. However, patients were asked to keep diaries to monitor compliance. Indeed, due to the pain-reducing effect of the tablets, physiotherapy could have led to an improvement in knee function.
Conclusions
In conclusion, our study suggests promising potential for oral hyaluronic acid and Boswellia serrata extract in managing knee osteoarthritis, albeit more extensive studies are required.
Despite several limitations, the present study showed that oral administration of hyaluronic acid and Boswellia serrata extract might have beneficial effects on patients with mild to moderate knee OA. Oral administration of HA and Boswellia serrata extract seems to decrease pain and improve knee function.
The effects of HA and Boswellia remain controversial, and long-term large prospective randomized studies are needed to clarify their therapeutic role. However, combined HA and Boswellia supplementation could reduce NSAID use in early knee OA and could be a valid means to prevent progressive degeneration of the articular hyaline cartilage and the consequent decrease in the anabolic reparative potential of chondrocytes and synoviocytes.
Conflict of Interest
E.M. received a research grant from River Pharma s.r.l. The other authors declare that they have no conflict of interest.
Informed Consent
All participants provided informed consent to participate in the study and to use their data for research purposes in accordance
with ethical standards.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
The study was approved on 15/12/2021 by the Ethics Committee of the “Sapienza” University with protocol number 367 SA_2021 of the Register of Opinions (REF. CE 6604_2021).
Funding
None.
Data Availability
Data are available upon request.
Authors’ Contributions
P.O., V.C. and G.R. were responsible for recruiting patients and collecting data.
A.C., P.O., G.R. and A.A. have interpreted the data and drafted the work.
E.M. and D.P. made substantial contributions to the conception of the work.
E.M., D.P. and N.M. have substantively revised the article.
A.C. and A.A. were responsible for statistical analysis and interpretation of data.
All authors also substantively revised the work and approved the submitted version. All authors read and approved the final manuscript.
ORCID ID
Edoardo Monaco: 0000-0003-2377-4829
References
1. Bannuru RR, Osani MC, Vaysbrot EE, Arden NK, Bennell K, Bierma-Zeinstra SMA, Kraus VB, Lohmander LS, Abbott JH, Bhandari M, Blanco FJ, Espinosa R, Haugen IK, Lin J, Mandl LA, Moilanen E, Nakamura N, Snyder-Mackler L, Trojian T, Underwood M, McAlindon TE. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage 2019; 27: 1578-1589.
2. Bannuru RR, Schmid CH, Kent DM, Vaysbrot EE, Wong JB, McAlindon TE. Comparative Effectiveness of Pharmacologic Interventions for Knee Osteoarthritis: A Systematic Review and Network Meta-analysis. Ann Intern Med 2015; 162: 46-54.
3. Cooper C, Rannou F, Richette P, Bruyère O, Al‐Daghri N, Altman RD, Brandi ML, Collaud Basset S, Herrero‐Beaumont G, Migliore A, Pavelka K, Uebelhart D, Reginster J. Use of Intraarticular Hyaluronic Acid in the Management of Knee Osteoarthritis in Clinical Practice. Arthritis Care Res (Hoboken) 2017; 69: 1287-1296.
4. He WW, Kuang MJ, Zhao J, Sun L, Lu B, Wang Y, Ma JX, Ma XL. Efficacy and safety of intraarticular hyaluronic acid and corticosteroid for knee osteoarthritis: A meta-analysis. Int J Surg 2017; 39: 95-103.
5. Nie L, Zhao K, Ruan J, Xue J. Effectiveness of Platelet-Rich Plasma in the Treatment of Knee Osteoarthritis: A Meta-analysis of Randomized Controlled Clinical Trials. Orthop J Sports Med 2021; 9: 2325967120973284.
6: Wei P, Bao R. Intra-Articular Mesenchymal Stem Cell Injection for Knee Osteoarthritis: Mechanisms and Clinical Evidence. Int J Mol Sci 2022; 24: 59.
7. Nagashima R, Tahara M, Akagi R, Watanabe S, Tozawa R, Ninomiya T, Sawai Y, Uzawa K, Sasho T. Consistency of differentially expressed genes in the subchondral bone of end-stage osteoarthritic knees. Joints 2023; 1: e167.
8. Majeed M, Majeed S, Narayanan NK, Nagabhushanam K. A pilot, randomized, double-blind, placebo-controlled trial to assess the safety and efficacy of a novel Boswellia serrata extract in the management of osteoarthritis of the knee. Phytother Res 2019; 33: 1457-1468.
9. Umar S, Umar K, Sarwar AHMG, Khan A, Ahmad N, Ahmad S, Katiyar CK, Husain SA, Khan HA. Boswellia serrata extract attenuates inflammatory mediators and oxidative stress in collagen induced arthritis. Phytomedicine 2014; 21: 847-856.
10. Kizhakkedath R. Clinical evaluation of a formulation containing Curcuma longa and Boswellia serrata extracts in the management of knee osteoarthritis. Mol Med Rep 2013; 8: 1542-1548.
11. Bowman S, Awad ME, Hamrick MW, Hunter M, Fulzele S. Recent advances in hyaluronic acid based therapy for osteoarthritis. Clin Transl Med 2018; 7: 6.
12. Tashiro T, Seino S, Sato T, Matsuoka R, Masuda Y, Fukui N. Oral administration of polymer hyaluronic acid alleviates symptoms of knee osteoarthritis: a double-blind, placebo-controlled study over a 12-month period. ScientificWorldJournal 2012; 2012: 167928.
13. Wang SJ, Wang YH, Huang LC. The effect of oral low molecular weight liquid hyaluronic acid combination with glucosamine and chondroitin on knee osteoarthritis patients with mild knee pain. Medicine (Baltimore) 2021; 100: 242-252.
14. Drogo P, Carrozzo A, Partezani Helito C, Zappalà G, Barelli GM, Argento G, Ferretti A, Monaco E. Magnetic resonance imaging evaluation of anterolateral ligament injuries and associated lesions in acute anterior cruciate ligament tears. Joints 2023; 1: e676.
15. Jackson GR, Lee JS, Asif S, Sachdev D, Mameri ES, Kaplan DJ, Khan ZA, Jawanda H, Batra AK, Obioha OA, Knapik DM, Familiari F, Laprade RF, Chahla J. Different suture configurations for transtibial pullout repair for medial meniscus root tears yield improved mid-term clinical outcomes: a systematic review. Joints 2023; 1: e796.
16. Balazs EA, Denlinger JL. Viscosupplementation: a new concept in the treatment of osteoarthritis. J Rheumatol Suppl 1993; 39: 3-9.
17. Ghosh P, Guidolin D. Potential mechanism of action of intra-articular hyaluronan therapy in osteoarthritis: are the effects molecular weight dependent? Semin Arthritis Rheum 2002; 32: 10-37.
18. Zhou PH, Liu SQ, Peng H. The effect of hyaluronic acid on IL-1beta-induced chondrocyte apoptosis in a rat model of osteoarthritis. J Orthop Res 2008; 26: 1643-1648.
19. Lùrati A, Laria A, Mazzocchi D, Re KA, Marrazza M, Scarpellini M. Effects of hyaluronic acid (HA) viscosupplementation on peripheral Th cells in knee and hip osteoarthritis. Osteoarthritis Cartilage 2015; 23: 88-93.
20: Yu G, Xiang W, Zhang T, Zeng L, Yang K, Li J. Effectiveness of Boswellia and Boswellia extract for osteoarthritis patients: a systematic review and meta-analysis. BMC Complement Med Ther 2020; 20: 225.
21. Ricci M, Micheloni GM, Berti M, Perusi F, Sambugaro E, Vecchini E, Magnan B. Clinical comparison of oral administration and viscosupplementation of hyaluronic acid (HA) in early knee osteoarthritis. Musculoskelet Surg 2017; 101: 45-49.
22. Jensen GS, Attridge VL, Lenninger MR, Benson KF. Oral intake of a liquid high-molecular-weight hyaluronan associated with relief of chronic pain and reduced use of pain medication: results of a randomized, placebo-controlled double-blind pilot study. J Med Food 2015; 18: 95-101.
23. Nelson FR, Zvirbulis RA, Zonca B, Li KW, Turner SM, Pasierb M, Wilton P, Martinez-Puig D, Wu W. The effects of an oral preparation containing hyaluronic acid (Oralvisc®) on obese knee osteoarthritis patients determined by pain, function, bradykinin, leptin, inflammatory cytokines, and heavy water analyses. Rheumatol Int 2015; 35: 43-52.
24. Oe M, Tashiro T, Yoshida H, Nishiyama H, Masuda Y, Maruyama K, Koikeda T, Maruya R, Fukui N. Oral hyaluronan relieves knee pain: a review. Nutr J 2016; 15: 11.
To cite this article
Potential benefits of oral hyaluronic acid and Boswellia serrata extract in patients with mild to moderate knee osteoarthritis
JOINTS 2024;
2: e1058
DOI: 10.26355/joints_20247_1058
Publication History
Submission date: 06 Dec 2023
Revised on: 04 Jan 2024
Accepted on: 11 Jul 2024
Published online: 31 Jul 2024